In Mexico, inequality in maternal healthcare is often explained by factors such as poverty, education, and access to services. However, a recent study suggests that a significant part of the problem stems from ethnic and racial discrimination within the healthcare system itself.
The research analyzed data from more than 72,000 Mexican women who had children between 2009 and 2023. To do this, they combined information collected by three editions of the National Survey of Demographic Dynamics (ENADID).
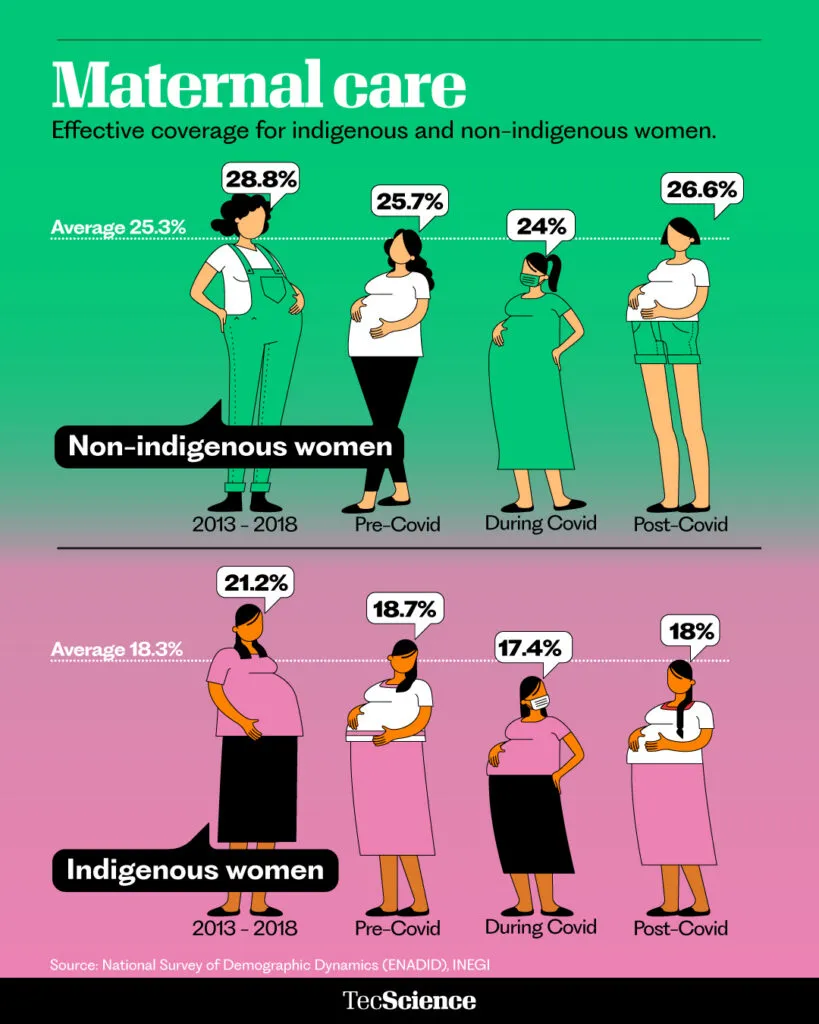
Its objective was to measure the effective coverage of maternal care, an indicator that considers not only whether a woman was treated in the health system but also whether she received the necessary care: adequate prenatal consultations, a delivery attended by trained personnel, postpartum follow-up, and the absence of serious complications.
Their results showed that, on average, this coverage was 25.3% for non-Indigenous women and only 18.3% for Indigenous women.
The gap appears at different points in the care process. 87.4% of non-Indigenous women received adequate prenatal care, compared to 76.6% of Indigenous women. The rate of attended childbirth reached 98% among non-Indigenous women, but fell to 84.6% among Indigenous women.
“We found structural discrimination in the medical care that Indigenous women receive in Mexico,” says Rocío García-Díaz, a research professor at the School of Social Sciences and Government of Tec de Monterrey and one of the authors of the article.
Taken together, these data suggest that many Indigenous women face obstacles throughout pregnancy, childbirth, and postpartum in receiving adequate care.
Obstetric Violence: What Part of that Gap is due to Racism and Discrimination?
Although some of these differences can be explained by the fact that women living in rural areas are further from health services and have less social security coverage, the researchers hypothesized that racism and discrimination are also a factor.
To test it, they used a statistical analysis called Oaxaca-Blinder decomposition that allows for the separation of how much of a difference between two groups —in this case Indigenous and non-Indigenous women— is explained by observable characteristics, such as education or income, and how much by unobservable factors, such as discrimination.
“In the absence of another explanation and being aware that there are forms of racism that affect indigenous populations, we attribute that difference to forms of discrimination,” says Sergio Meneses, a researcher at the National Institute of Public Health and one of the authors of the research.
The results indicated that 51.7% of the gap in maternal care can be attributed to ethnic and racial discrimination, 30.8% is related to socioeconomic differences, and 17.5% to the interaction between both factors.
This means that more than half of the inequality in care is not explained solely by social conditions, but by how the health system responds to Indigenous women.
According to Meneses, some people try to attribute these differences to the so-called customs and traditions of Indigenous populations, such as being treated by midwives or preferring not to go to a hospital.
However, for the researcher, it is clear that a significant part is due to systematic mechanisms of exclusion, marginalization, and oppression.
“In general, being racist is shameful, something we don’t want to admit,” Meneses reflects. “But the truth is that in practice, of course there are spaces where forms of exclusion toward Indigenous populations are systematically practiced.”
Structural Inequalities
Universal health coverage is one of the main goals of the United Nations (UN) and seeks to ensure that all people can access quality health services without facing economic barriers.
However, according to the results of this study, Mexico is still far from achieving equity in the health system.
Although not all the difference in access is due to discrimination and racism, it is clearly a very important factor.
Their results also report that 49.4% of Indigenous women said they had some health problem during pregnancy, while 33.7% of non-Indigenous women did.
“One challenge for public health is how to bring indigenous women closer to the health system at this vulnerable stage,” says García-Díaz.
The study also notes that some changes in public policy coincided with setbacks in coverage. One of these was the elimination of Seguro Popular in 2019, which had been designed to expand access to health services among the population without social security.
This suggests that universal coverage policies not only depend on expanding infrastructure or financing, but also require addressing the structural inequalities that affect certain groups.
Beyond Universal Coverage
The authors point out that in Mexico and Latin America, social hierarchies based on racial ideas have historically contributed to the marginalization of Indigenous populations. This is reflected in their lack of access to education, land, and basic services, as well as their lower incomes.
In the health system, this can manifest itself in lower quality of care, a lack of culturally appropriate services, or discrimination by medical staff.
Although progress has been made in reducing inequality in maternal care between Indigenous and non-Indigenous women, it still persists.
To resolve this, it is necessary to understand this reality and confront it. “All of us who are part of the healthcare system, including administrative and security personnel, must keep in mind that providing dignified treatment to all people is a goal, not an add-on.”
Thus, expanding health service coverage is not enough if the structural factors that generate this inequality are not addressed. Continued efforts to guarantee access to healthcare for Indigenous women are essential.
“Mexico has a large percentage Indigenous population,” says García-Díaz. “Surely the government will be interested in making the pregnancy process as inclusive and equitable as possible for Mexican women, regardless of whether they are Indigenous or not.”
Did you find this story interesting? Would you like to publish it? Contact our content editor for more information: marianaleonm@tec.mx