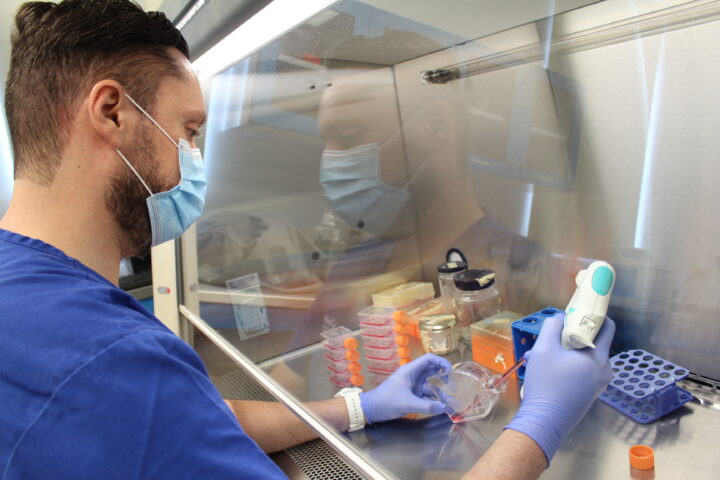
In December 2022, Andrés –a transgender man who has asked TecScience to protect his real name– attended clinical laboratories in Mexico City to have an ultrasound to ensure that there were no abnormalities in his mammary glands before undergoing subcutaneous mastectomy as part of his gender reaffirmation process.
“Normally, it would have taken 25 minutes, but it took an hour and a half due to a lack of staff training. They took me to a room and asked me more questions,” says Andrés. “They spoke to me using she/her pronouns and treated me in a derogatory manner.”
Before leaving, his mother, who was accompanying him, filed a complaint with the place’s supervisors for discrimination.
“They told me, in a loud voice, that it was my fault because I hadn’t shaved before my appointment. It was embarrassing; all the people who were waiting for their turn found out.”
Being treated like that left him feeling uneasy. “Since then, if I need to go to a doctor, I make sure through people I know that they are allies of trans and queer people.”
His case is just one of many examples of how medical and health personnel sometimes discriminate against members of the LGBTIQA+ community.
Medical Care for the LGBTIQA+ Community
Five years before Andrés’ case, the Ministry of Health in Mexico published the first Protocol for Access without Discrimination to the Provision of Health Care Services for LGBTTI people.
There are many other guidelines from health institutions focused on providing quality care to members of this community, but discrimination is still common.
“I think it starts with the pronouns; we should ask them [at the beginning of the consultation], but it is something we don’t do,” says Amairany Vega, a surgeon at the School of Medicine and Health Sciences at Tec de Monterrey.
Vega, a bisexual woman, led a chapter in the book The Lifelong Learning of Health Professionals: Continuing Education and Professional Development, on how to raise awareness about community care in future generations.
She and her colleagues explain that discrimination against this population by health personnel can take many forms.
Among them are not using the appropriate pronouns, assuming the sexual orientation of patients due to their behavior, making judgments regarding their sexual activity, and omitting questions due to ignorance of other sexual practices that are different from heterosexual vaginal intercourse.
This can result in misdiagnoses, refusal of certain exams or tests, or prejudiced attribution of an illness.
“It is still assumed that some diseases, such as HIV, are transmitted more between homosexual men, but there is no scientific support for this,” explains Vega.
One of the most severe consequences of this discrimination is that people who belong to this community prefer not to go to the doctor.
“My experience is similar to that of many trans people who try to minimize their contact with any type of doctor,” says Andrés.
In Mexico, compared to the rest of the population, 5.9% more LGBTIQA+ people seek medical care in the private sector, and 2.1% do not seek it in any setting, according to the National Survey on Sexual and Gender Diversity (ENDISEG).
The First Step Towards Non-Discrimination is in the Academy
According to Vega, it all starts in school, when medical students learn about diseases’ theoretical and practical aspects.
“I think that, even though there is already research on the matter, there is still a gap between what is said and what is done,” says Pilar González, Leader of Preventive and Training Strategies at the Center for the Recognition of Human Dignity (CRDH) of TecSalud.
Therefore, teaching the medical community about how to care for LGBTQI+ people empathically continues to depend on teachers or students who are sensitive to the issue.
“The medical discipline has very patriarchal, simplistic, and binaristic features. It was established as a rigorous science, but is not self-critical; it remains blind and stubborn to admit the relevance of social sciences in its study. There is also a remnant of some religious values that are too focused on sexuality,” González points out.
Vega adds that non-heterosexual practices are minimized “as if they were an exception, but they are not.”
In Mexico, 5.1% of the population aged 15 years or older identifies as part of the LGBTIQA+ community, according to ENDISEG.
Therefore, updating study plans and preparing those who teach is essential. “Currently, the faculty is not qualified to teach courses on these topics. That effort is also needed,” says Vega.
How to Eradicate Discrimination Against the LGBTIQA+ Community in the Medical Environment
To eradicate poor care and discrimination towards the LGBTQI+ community by health personnel, a coordinated effort is needed from various spheres of society, but, above all, from decision makers.
“It is urgent to raise awareness among the people making the decisions, both in schools and in medical practice,” says González.
Representing LGBTIQA+ people within hospitals, medical schools, and practices is equally important.
“Currently, [hospitals and medical scenarios] are not such safe spaces for them to demonstrate their diversity. Mechanisms need to be put in place to protect those who are vocal about their sexual or gender identity,” she adds.
Efforts must also be focused on encouraging scientific research with a gender perspective. “The stigmas about gender-based dissidence are powerful; they must be broken with evidence,” says González.
It is also key to invite people from the medical community to seek to improve their relationships with their patients and their care for this community.
“People come for consultation when they are vulnerable, sick or in pain,” says González. “We should be particularly empathetic toward everyone.”
Although medical professionals often have complicated schedules, it is time to prioritize the care of the most vulnerable communities.
“I know that sometimes they don’t have the time to do these trainings. I don’t think they do it maliciously, but they can change how you go to the doctor and whether you go or not in the first place,” says Andrés.
Although the panorama sounds complex, according to González and Vega, it is encouraging that new generations seek to break with the care paradigms that have prevailed until now.
“As health professionals, we are important in treating diseases, but also in accompanying the people we care for,” says Vega.
Were you interested in this story? Do you want to publish it? Contact our content editor to learn more marianaleonm@tec.mx