The pain and fatigue started one October afternoon last year. Although unusual for me, I tried to convince myself it was just normal soreness from exercise or work overload. But almost overnight, the discomfort turned into torment.
The only way I can describe it is like needles piercing my joints, a heavy pressure on my lower back, and the eerie feeling that my eyes were being pulled backward.
At the time, I was living in Guadalajara, Jalisco, where daily headlines warned of a dengue crisis. As a science journalist, it didn’t take long to put the pieces together: I was in the middle of a record-breaking outbreak, exposed to the mosquito that transmits the disease, and showing several of its telltale symptoms.
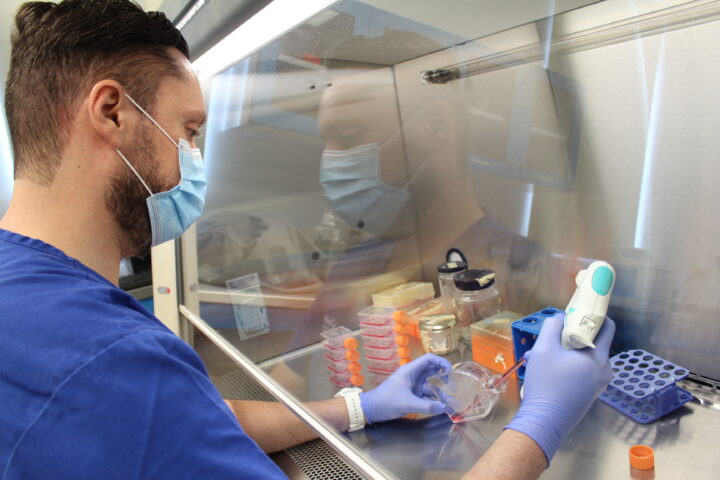
After ordering a confirmatory antigen test and a complete blood count to monitor warning signs, my doctor prescribed isolation, near-total rest, fever reducers, and plenty of fluids.
Like most cases, mine was considered mild—but it still knocked me out for two weeks. And when I finally felt like myself again, a month later, I was left with far more questions than answers.
Who Does Dengue Affect?
Just a few years ago, the idea that dengue could reach mountain regions or temperate latitudes seemed impossible. Yet today it’s no longer a disease of impoverished tropical areas—it’s a global threat that, according to the World Health Organization (WHO), now puts half of humanity at risk.
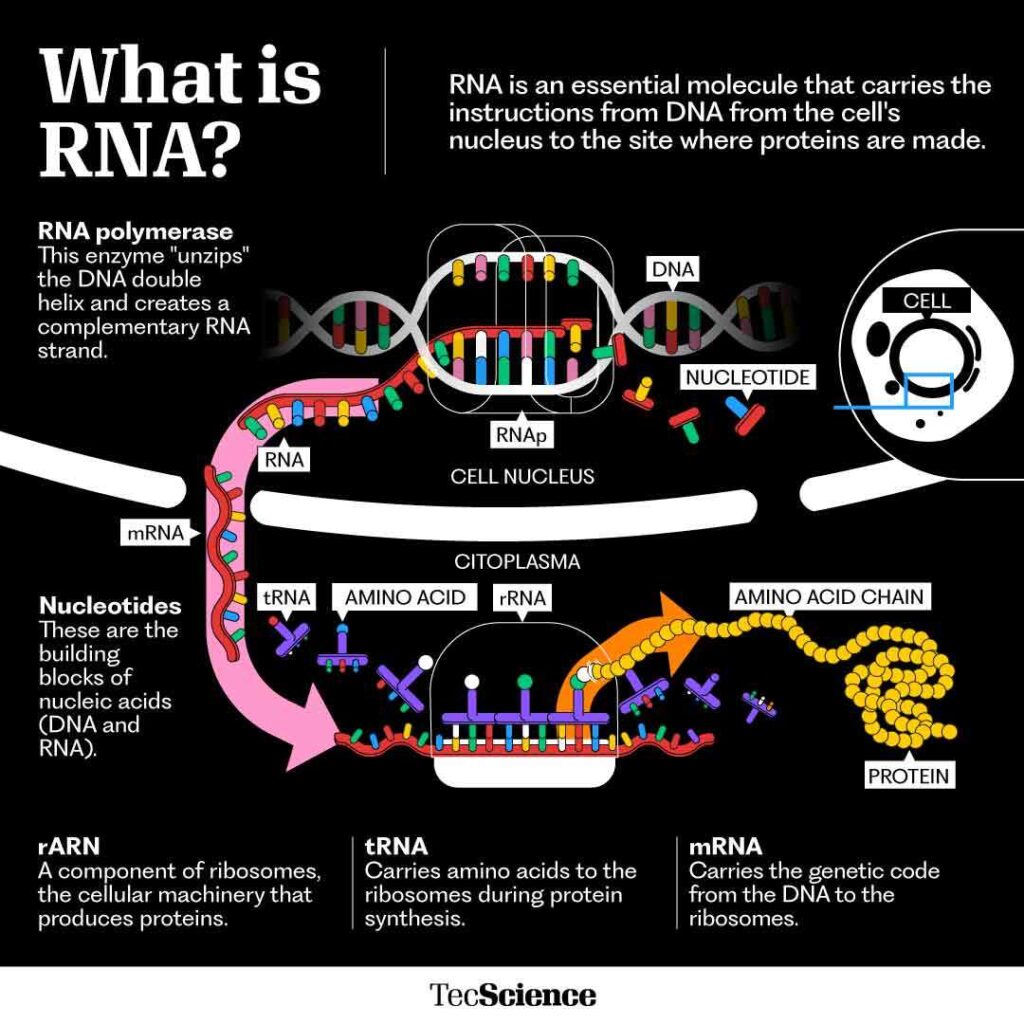
“Dengue is an infectious disease caused by an RNA virus transmitted through the bite of female Aedes aegypti or Aedes albopictus mosquitoes,” explains Mariana Merlo, president of the Infectology Society of Jalisco.
There are four viral serotypes, and catching one of them doesn’t grant immunity against the others. On the contrary, as Merlo points out, “over the course of a lifetime, any patient can be infected with all four types of dengue, and each reinfection increases the risk of severe disease by 3.5 times.”
To make matters worse, the fatality rate is rising. Biomedical researcher Victoria Pando Robles, from Mexico’s National Institute of Public Health, notes that “in 2010 it was under 1%, but by 2020 it had climbed to nearly 3%.”
She also highlights a troubling trend: while severe cases remain more common among pregnant women, older adults, and patients with comorbidities, “we’re seeing a significant increase among people under 20.”
Why haven’t we controlled it?
For decades, the dominant belief was that eliminating mosquito vectors would solve the dengue problem. As a result, public health strategies relied heavily on the mass use of insecticides.
But José Pablo Liedo, a researcher at El Colegio de la Frontera Sur and recipient of the EXATEC award, is one of its most vocal critics.
“All the evidence has shown the ineffectiveness of the methods we’ve been using,” he warns.
Overuse of insecticides has serious consequences: they often fail to kill eggs or larvae, create a false sense of security, wipe out non-pest species, pollute the environment, and drive resistance.
Take DDT, for example. When its widespread use began in 1946, resistant mosquito populations were already documented by the following year.
Pando Robles adds that dengue is far more complex than just the mosquito itself. Human mobility, she explains, is crucial: “Mosquitoes fly only 200 to 600 meters—not even across a city block. The ones really carrying the virus around are people, because we move much farther.”
Liedo, meanwhile, underscores the role of rapid urbanization. The dengue mosquito is an urban insect, he says: “Outside of where humans live, there’s no Aedes aegypti. Places with heavy rainfall but poor water infrastructure, sewage systems, and potable water are hotspots for this kind of disease.”
And then there’s climate change, which is expanding the mosquito’s reach.
“Aedes albopictus—which also transmits dengue, chikungunya, and Zika—is now reported in southern Europe: in Italy, in southern France. That had never happened before,” Liedo says. And unless action is taken, projections suggest an even grimmer future. A 2019 study using climate models found that under the worst-case scenarios, nearly 1 billion more people could be exposed to dengue this century.
Can we ever eradicate it?
The shortcomings of traditional strategies have prompted science to adopt new, multifaceted approaches. Among the most promising are two vector-control methods:
- The Sterile Insect Technique (SIT): Instead of killing mosquitoes, it reduces their reproduction. Males are bred in labs, sterilized with radiation, and released en masse to mate with wild females. With no offspring, populations gradually shrink. Pilot projects in Singapore and Cuba have shown both safety and potential.
- Wolbachia bacteria: By deliberately introducing Wolbachia into mosquitoes, the insects lose their ability to transmit dengue. Liedo refers to this as a “replacement technique” that has proven effective in projects in Australia. Still, the risk remains that the bacteria could lose its virus-blocking ability—so some specialists suggest combining it with SIT.
On another front, vaccines are beginning to offer hope. Merlo specifically points to QDENGA, now in use in countries such as Brazil, with a 60% efficacy rate. Unlike earlier options, it doesn’t require prior infection for effectiveness.
Liedo concedes that eradicating dengue may be unrealistic. But with an integrated toolkit, he believes its impact can be significantly reduced. Pando Robles insists the real danger is complacency: we can’t afford to accept dengue as a disease that “just happens to everyone.”
Prevention, ultimately, begins at home—clearing patios, turning over containers, and eliminating standing water where mosquitoes breed. Only through a combination of cutting-edge science and collective awareness can we hope to contain an epidemic that no longer respects borders.
Interested in this story? Want to publish it? Contact our content editor at marianaleonm@tec.mx