
By Valeria Atehortúa, Daniela Mendoza, Ximena Palacios, Rubén Ávila, Sarah Arcipreste, Jesús Alí Montes and Natalia Rivera / Ciencia Amateur.
Contributing author Jorge Membrillo Hernández
Every year, thousands of patients in Mexico are admitted to hospitals for treatment, only to develop infections unrelated to the condition that brought them there. Known as healthcare-associated infections (HAIs), these infections remain a major public health challenge.
In 2024 alone, nearly 13,000 HAIs were reported in Mexico City, with an estimated 29% mortality rate.
One of the leading drivers of these infections is the growth of bacterial communities on the surfaces of medical devices such as catheters, urinary tubes, and implants. These communities—known as biofilms—have drawn increasing attention, particularly after reports during the COVID-19 pandemic showed that many hospitalized patients with COVID-19 or atypical pneumonia also developed biofilm-associated infections.
What are biofilms, and how do they form?
Since the days of pioneering microbiologists such as Louis Pasteur and Robert Koch, microbiology has largely portrayed bacteria as free-floating organisms growing in flasks, liquid cultures, or Petri dishes under carefully controlled laboratory conditions.
Outside the lab, however, bacteria rarely live alone. In nature, they typically attach to surfaces or exist within liquid environments. They inhabit the human body—from the skin and nails to internal organs and the gut microbiome.
Over the past three decades, researchers have uncovered the remarkably social behavior of bacteria. Rather than existing as isolated cells, many species organize into biofilms—highly structured microbial communities encased in a self-produced protective matrix that shields them from environmental threats.
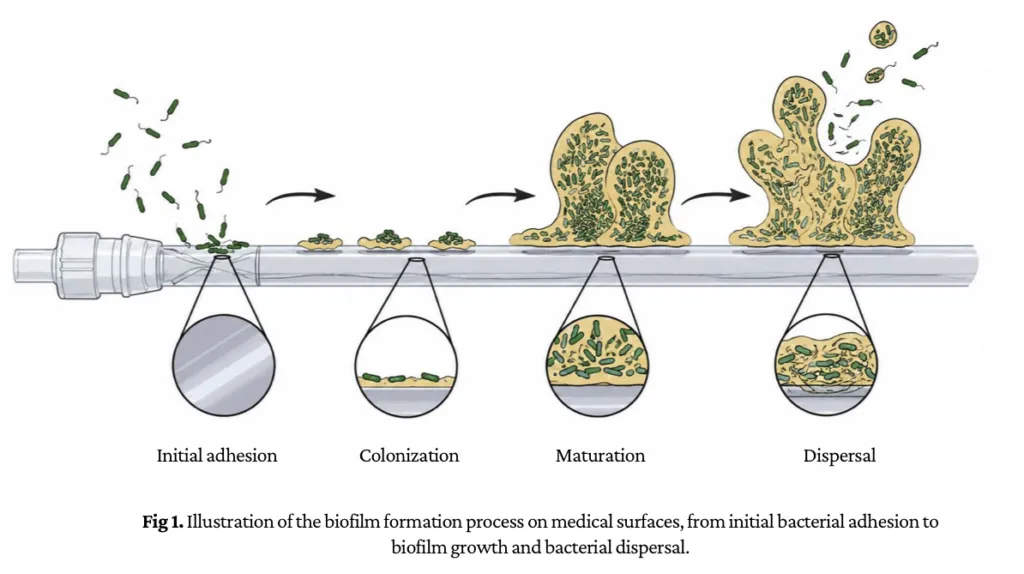
This protective matrix not only gives biofilms their structural integrity but also shields them from external threats, including antibiotics and a patient’s immune system. The formation of these microbial communities is regulated by cell-to-cell communication mechanisms such as quorum sensing, which enables bacteria to coordinate their collective behavior.
If bacteria can dramatically increase their resistance to antibiotics, what happens when disease-causing microbes colonize the surfaces of medical devices used in hospitalized patients? Over the past decade, researchers have shown that biofilms forming on biomedical surfaces can lead to persistent infections that are difficult to eradicate—and, in severe cases, can become life-threatening.
Researchers still do not fully understand how the physicochemical properties of medical-grade materials influence biofilm formation over time. Manufacturers continue to develop new polymers designed for hospital use while reducing bacterial attachment, yet many questions remain about how bacteria interact with the surfaces of medical devices throughout their life cycle.
The challenge for medical devices
When bacterial communities attach to catheters, heart valves, pacemakers, and other implanted devices, they can trigger persistent infections that are notoriously difficult to treat. Their protective structure makes them highly resistant to antibiotics while allowing them to evade the body’s immune defenses, increasing the risk of serious complications.
Materials science has become a critical part of addressing this problem.
Medical-grade polymers such as polyamide 12 (PA12) are widely used to manufacture catheters, while polyetheretherketone (PEEK), a high-performance semicrystalline thermoplastic, is used not only in medical devices but also in aerospace and automotive applications.
At Tec de Monterrey, researchers are using PEEK and PA12 beads to develop a reproducible protocol for measuring biofilm growth over time and determining how the surface properties of these polymers affect bacterial attachment and biofilm development.
The team cultured bacteria in PVC microplates containing beads made from each polymer.
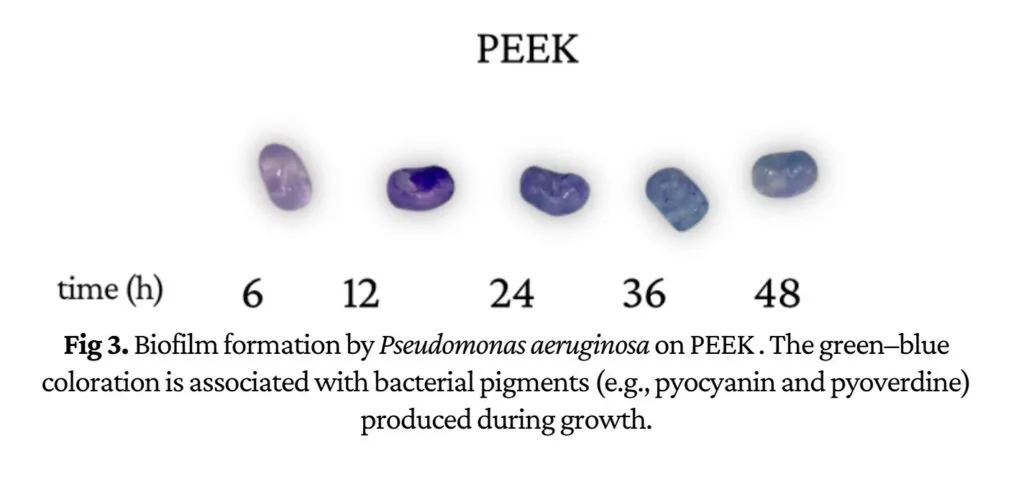
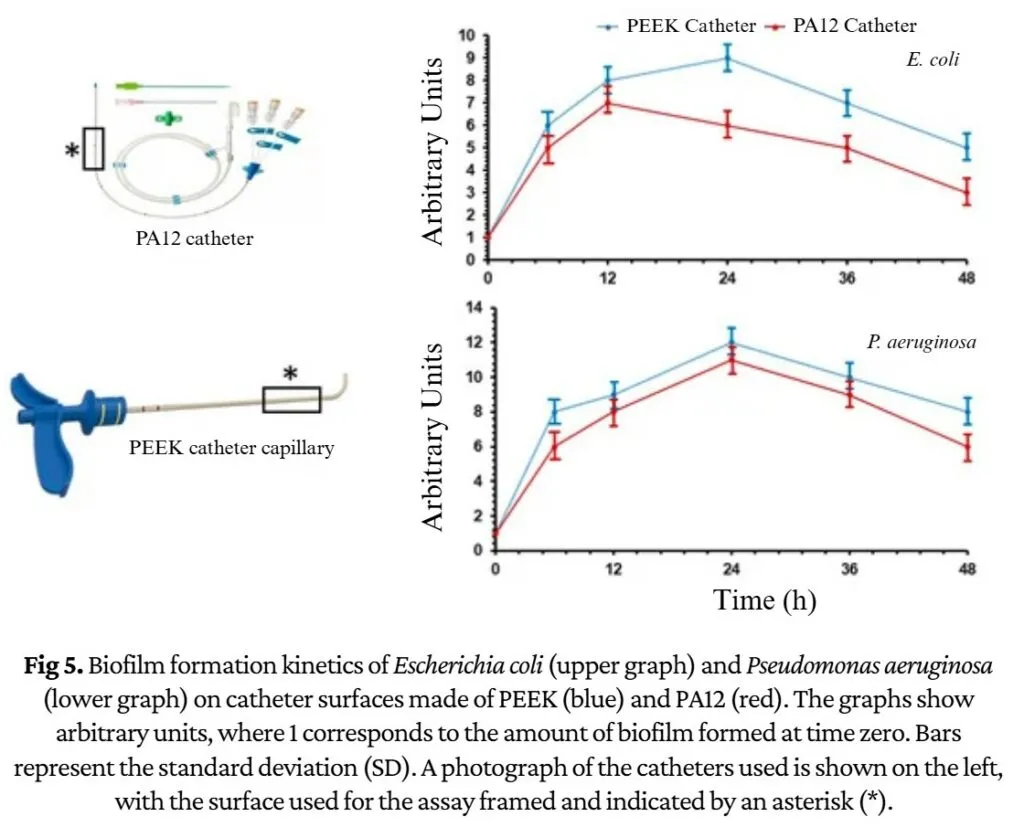
Their results showed that both Escherichia coli and Pseudomonas aeruginosa readily formed biofilms on both materials, although their growth patterns differed significantly. E. coli reached peak biofilm formation after 12 hours on PA12 but required 24 hours on PEEK. P. aeruginosa, meanwhile, produced less biofilm on PA12 and reached its maximum growth after 24 hours on PEEK.
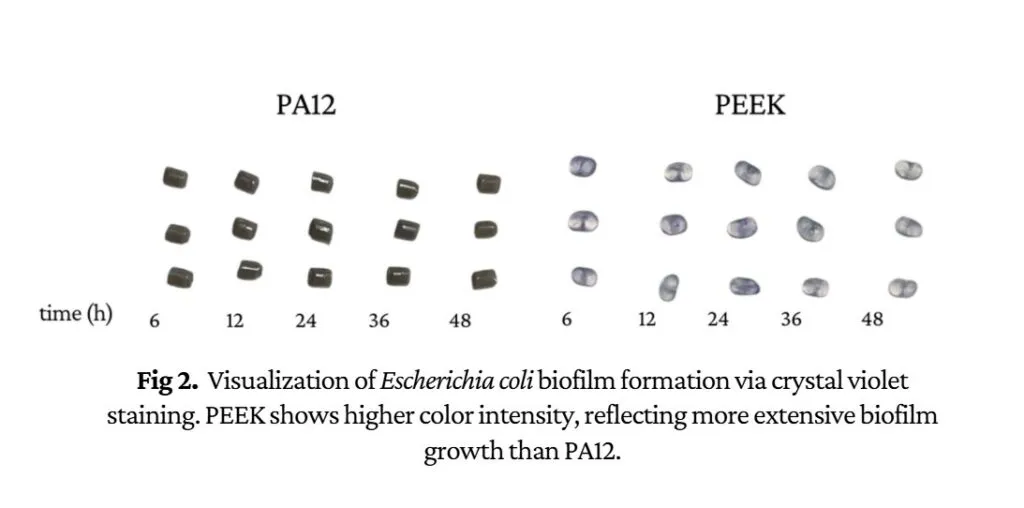
Overall, PEEK consistently promoted greater biofilm formation than PA12, suggesting that its surface properties provide a more favorable environment for bacterial attachment.
These findings are especially relevant given that millions of intravascular catheters are used worldwide each year, and even a small proportion becoming colonized can result in bloodstream infections. Such infections are closely linked to the ability of bacteria to adhere to device surfaces and develop biofilms, dramatically increasing their resistance to treatment.
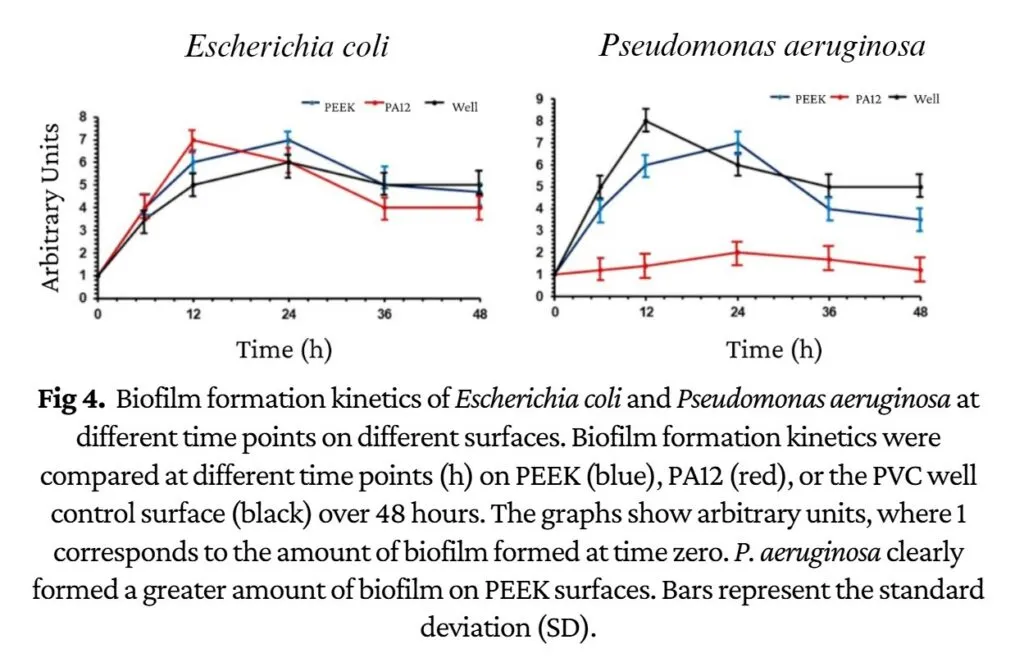
The researchers also evaluated commercial catheter materials. In most cases, biofilm biomass increased rapidly during the first 24 hours, except for E. coli growing on PA12, which peaked after 12 hours. Biofilm levels then declined, likely because of nutrient depletion, bacterial dispersal, or cell death.
The results indicate that biofilms reach maturity early in their development and identify the first 12 hours as the critical window during which bacterial colonization becomes established.
Toward safer biomaterials
The study highlights the importance of preventing bacterial attachment during the earliest stages of colonization and shows that material selection can strongly influence biofilm formation.
Researchers demonstrated that Pseudomonas aeruginosa and Escherichia coli—two of the pathogens most frequently linked to hospital-acquired infections—can readily grow on medical-grade polymers such as PEEK and PA12. They also found that PEEK is more susceptible to biofilm accumulation than PA12.
A better understanding of how bacteria interact with biomaterials could help engineers develop medical devices that are more resistant to bacterial colonization, ultimately reducing hospital-acquired infections and improving patient outcomes.
.
References
- Mejía-Manzano, L. A., Vázquez-Villegas, P., Prado-Cervantes, L. V., Franco-Gómez, K. X., Carbajal-Ocaña, S., Sotelo-Cortés, D. L., Atehortúa-Benítez, V., Delgado-Rodríguez, M., & Membrillo-Hernández, J. (2023). Advances in material modification with smart functional polymers for combating biofilms in biomedical applications. Polymers, 15(14), 3021.
- VESTAMID® L – polyamide 12 – Evonik Industries. (2024, May 24). https://www.vestamid.com/en/products-services/VESTAMID-L
- ALBIS – VESTAKEEP® PEEK. (n.d.). https://www.albis.com/en/products/products-brands/evonik/vestakeep?utm_source=chatgpt.com
- S. Carbajal-Ocaña et al., «In Vitro Biofilm Formation Kinetics of Pseudomonas aeruginosa and Escherichia coli on Medical-Grade Polyether Ether Ketone (PEEK) and Polyamide 12 (PA12) Polymers,» Hygiene, vol. 5, p. 32, ago. 2025
Authors
Valeria Atehortúa-Benítez and Daniela Mendoza Lozano, Biomedical Engineering students.
Ximena Citlali Palacios-Cota, Rubén Ávila-Garnica, Sarah Arcipreste-García, and Jesús Alí Montes-Zúñiga, Biotechnology Engineering students.
Natalia Rivera-Melo, Bachelor’s degree student in Biosciences.
This article was reviewed by Jorge Membrillo Hernández, research professor at Tecnológico de Monterrey, Mexico City campus, and member of the Institute for the Future of Education.